| Hoofdstuk 47 - Paragraaf 1 |
47. Houding en keelstand

47.1 Houding en keelstand
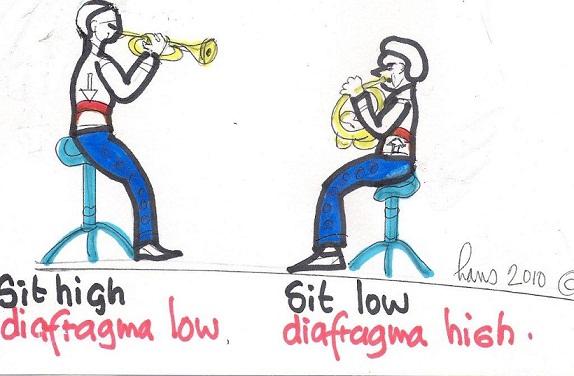
Als je hoger zit heb je meer lucht, omdat de druk vanuit de buikholte lager is. Het middenrif kan verder naar omlaag worden aangespannen. De koepel komt dus lager te staan waardoor de resonantieruimte in de longen groter wordt.
Klik op het plaatje om te vergroten.
Als je lager en dieper gaat zitten wordt inademen moeilijker omdat de koepel veel hoger komt te staan en de resonantieruimte in de longen kleiner wordt.

Klik op het plaatje om te vergroten.
1. Als je je lichaamsgewicht naar de voorvoet verplaatst, zullen de rug- en nekspieren grotere inspanning moeten verrichten als bij 3, de normale stand.
Hierdoor zal de onderkaak naar achteren bewegen en de keel zich vernauwen. Hierdoor wordt de toon geknepen.
2. Als je je gewicht naar de hiel verplaatst zal de rug boller worden en het hoofd naar voren worden getrokken en de onderkaak naar achteren. Een gespannen en geknepen situatie ontstaat.
3. Als je je gewicht goed verdeelt over de gehele voet, zul je de kruin het beste kunnen strekken en zal de onderkaak makkelijker naar voren gaan. Dat is nodig om een goede druk van het mondstuk op de onderkaak te krijgen. Ook zal daardoor de keel beter open gaan.
Spirometric forced expiratory volumes measured in the standing versus the sitting posture.
Townsend MC.
To date, only one study has empirically examined the effects of sitting versus standing posture on the spirometric forced expiratory volumes. Because of design limitations, the small excess of sitting over standing values found in that study may have been due to a positive testing order effect. Using a crossover design, the present study of 90 middle-aged male subjects alternated the sitting-standing and standing-sitting testing sequence between subjects to avoid confounding by testing order effects. The major findings were that forced expiratory volumes in one and in six seconds and forced vital capacity were significantly larger (p less than 0.001) in the standing than in the sitting posture, with mean standing minus sitting differences ranging from +0.06 to +0.08 L for the 3 indexes. The larger expired volumes measured in the standing position in this study were probably due to the subjects taking slightly larger inspirations in this posture than in the sitting position.
PMID: 6742596 [PubMed - indexed for MEDLINE]
Chest. 1976 Jul;70(1):17-20.
A comparison of spirometric values with subjects in standing and sitting positions.
Pierson DJ, Dick NP, Petty TL.
Spirograms obtained from 235 subjects in standing and sitting positions revealed small differences for the forced vital capacity (FVC) and forced expiratory volume in one second (FEV1). No statistically significant differences were found for the mean forced expiratory flow during the middle half of the FVC (FEF25-75%, or maximal midexpiratory flow) and FEV1/FVC. Sitting values were, on the average, higher for determinations greater than FVC of 2.14 L, FEV1 of 1.68 L, FEF25-75% of 2.16 L/sec, and FEV1/FVC of 75.7 percent. On the average, subjects with less than these values performed slightly better in the standing position.
PMID: 1277923 [PubMed - indexed for MEDLINE]
Effect of different sitting postures on lung capacity, expiratory flow, and lumbar lordosis.
Lin F, Parthasarathy S, Taylor SJ, Pucci D, Hendrix RW, Makhsous M.
Department of Physical Therapy and Human Movement Sciences, Northwestern University, Chicago, IL, USA.
OBJECTIVE: To investigate the effect of sitting posture on lung capacity and expiratory flow (LC-EF) and lumbar lordosis. DESIGN: Repeated measures on 1 group of subjects in 4 postures. SETTING: Laboratory. PARTICIPANTS: Seventy able-bodied volunteers. INTERVENTIONS: Postures were assumed randomly: normal, with full ischial support and flat lumbar support; slumped, with the pelvis positioned in the middle of seat while leaning against the backrest; against the back part of the seat without ischial support (WO-BPS), with partially removed ischial support and an enhanced lumbar support; and standing. MAIN OUTCOME MEASURES: For LC-EF, forced vital capacity, maximum forced expiratory flow, forced expiratory volume in 1 second, and peak expiratory flow; and lumbar lordosis. RESULTS: All LC-EF measures in standing were significantly superior to those in slumped and normal sitting, and 4 measures were significantly higher than in WO-BPS. In slumped sitting, LC-EF significantly decreased from that in normal sitting. WO-BPS sitting significantly increased 4 of the LC-EF measures from those in the normal sitting. Lumbar lordosis was the highest in standing and progressively decreased in WO-BPS, normal, and slumped sitting. CONCLUSIONS: Slumped sitting significantly decreased LC-EF and lumbar lordosis. Because it increases the lumbar lordosis and promotes LC-EF, the WO-BPS posture may be a better seating option for people sitting for a prolonged time.
PMID: 16571389 [PubMed - indexed for MEDLINE]
|